MENGIMBAS PERJUANGAN 2008
DIBAWAH ADALAH POSTING SAYA 10 TAHUN LALU PADA 18 NOV 2008 !
Salam sejahtera semua rakan perjuangan,
Sudah tiba masanya kita mengubah corak langkah dasar perjuangan dalam pembangunan profesion keseluruhannya. Kesatuan telah memainkan peranan baik selama ini dan satu usaha terbesar yang dilakukan selain usaha2 lampau ialah penukaran title ke Pen.Pegawai Farmasi. Walaupun secara peribadi saya telah jelaskan tidak menyokong gelaran ini.
Tetapi kejayaan tetap telah dilakukan oleh Kesatuan dan sekurang-kurangnya telah meningkatkan imej kita ke satu tahap yang lebih dari sebelumnya.
Pegawai-pegawai juga sudah mula menerima kita dengan gelaran baru ini.
Ingin saya mengolah kembali artikel saya sebelum ini berkaitan gelaran baru ini. Satu kajian yang komprehensif mengenai pro dan kontra pemilihan gelaran harus dilakukan dahulu lagi dengan mengambil kira sebab dan akibat serta mengambil kira hala tuju Pegawai Farmasi kerana jika kita mengetahui halatuju mereka, kita akan juga dapat menyesuaikan diri dengan perubahan besar yang bakal berlaku kepada sistem perkhidmatan Farmasi. Mungkin ramai yang baca akan marah terutama AJK kesatuan. Saya tidak akan siarkan artikel tanpa sebab munasabah dan selepas mendapat maklumat lengkap dari mereka-mereka yang berilmu tinggi.
Saya amat dekat dan selalu berbincang dengan para Pengajar di Kolej, Pen.Setiausaha Bhg Latihan, anggota HKL, Persatuan dan beberapa ahli-ahli dinamik PPF dimana mereka kerap menerima maklumat2 terkini semasa mesyuarat peringkat atasan. Pandangan saya bukan pandangan peribadi tetapi mewakili juga para cendiakiawan PPF dan bekas PPF yang telah menjadi Pengajar dan Pen.Setiausaha (BPL). Mereka benar2 kecewa dengan pemilihan gelaran baru ini. Ini adalah fakta sebenar.
Kenapakah gelaran baru ini tidak dipersetujui? Inilah persoalan yang semua harus ketahui. Kita tidak boleh mengelak dari hakikat bahawa profesion kita sebenarnya adalah kumpulan sokongan kepada Pharmacist. Jika dahulu memang kita berada dibarisan hadapan, tetapi peranan tersebut diambil oleh Pegawai kerana ia memang tugas mereka sebenarnya. Kita tidak harus rasa terancam dalam hal ini. Di Malaysia peranan tersebut sangat lambat dikendalikan secara langsung oleh Pegawai Farmasi. Maksud disini ialah berperanan di perkhidmatan kaunter bersama-sama juga dengan Penolong Pegawai Farmasi bila diperlukan.
Untuk makluman semua, dalam Persidangan Pen.Pegawai Farmasi Perak pada 31 Oktober lepas, saya amat terharu dengan taklimat oleh TPKN(F) Tn.Hj.Ruhaiyem yang banyak menyentuh pembangunan profesion kita sedalam-dalamnya. Beliau ada menyebut tentang kesilapan Pegawai Farmasi sendiri yang memilih gelaran yang salah iaitu "Pegawai Farmasi" yang mana menurut beliau sepatutnya memilih gelaran "Ahli Farmasi". Beliau mengatakan bahawa "sudahlah kita tersalah pilih nama, u all pun ikut belakang nama Pen.Pegawai Farmasi"! Menurut beliau gelaran "Pegawai Farmasi" sendiri mirip kepada tugas2 pentadbiran dan tidak mencerminkan tugas klinikal. Seterusnya beliau mencadangkan kita memilih gelaran teknikal seperti diluar negara sebagaimana yang saya cadangkan.
Ini adalah kerana sebenarnya kita dalam profesion ini tiada "HAK" sendiri terhadap satu-satu tugas atau kepakaran yang anggota lain boleh lakukan. Kalau dahulu kita pakar dalam penyediaan dan pembancuhan ubatan(Unit Galenikal) penyediaan I/V, penyediaan ubat mata dan telinga, penyediaan losyen dan krim/ointment dll, tapi tugas tersebut tidak lagi dilakukan kecuali untuk extemporanues atau persediaan seperti Mist.Potasium chloride, Scholl solution, Mist.Expectorant Stimulant dll bila perlu. Inilah yang selalu ditekankan oleh YDP Persatuan iaitu Tn.Hj.Kamaruddin "berkaitan hak keatas tugas dan kepakaran" dalam ucapan dasar beliau dahulu dalam AGM 2007 di Kuching.
Kita boleh mendapat hak tersebut sekiranya memilih satu gelaran yang bersifat teknikal. Seterusnya kita juga boleh mendapat Ijazah yang relevan iaitu Degree in Pharmaceutical Technology atau Pharmaceutical science. Ijazah ini memang berjalan di USA dan Eropah kepada Pharmacy Technician. Di USA para Pharmacy Technician yang menghabiskan Ijazah Pharmacy Technology akan di gelar Pharmacy Technologist!
Bilangan credit hours pembelajaran di USA adalah hampir sama dengan Diploma Farmasi kita iaitu 96 credit hrs.
Harus diberi perhatian bahawa pembelajaran dan gelaran jawatan mestilah seimbang dan relevan. Jika ingin menjadi Pegawai Farmasi, PPF boleh memohon saluran biasa yang disediakan jika layak. Kepada lain-lain PPF berdiploma bolehlah memohon Ijazah ini sekiranya telah diiktiraf.
Satu kajian dan bengkel boleh diusahakan untuk mengembangkan skop kerja yang mendalam dalam bidang teknikal terutama dalam TPN, CDR, Farmasi Bekalan Wad, RadioFarmasi, Perolehan & Bekalan, Home Medication Review dll skop dimana tugas-tiugas ini boleh dipisahkan antara klinikal dan teknikal. Jika gelaran kita pen.Pegawai farmasi, skop ini tidak boleh dipisahkan kerana apa2 tugas yang dilakukan oleh Pegawai, kita juga lakukan. inilah yang tidak digemari oleh mereka dengan gelaran baru ini.
Cuba bayangkan jika gelaran baru kita adalah Juruteknoloji Farmasi atau Teknologis Farmasi, gelaran ini merujuk kepada kepakaran dalam bidang berkaitan dan bukan pembantu kepada sesiapa. Kita juga berpeluang meningkat dalam Gred dari U29 hingga Gred U54 jika dengan nama gelaran ini (jika ada Ijazah dengan usaha mendapatkannya). Tetapi dengan nama Pen.Pegawai Farmasi bolehkah digelar Pen.Pegawai Farmasi U41? PPF telah di'seal' dibawah U41 dengan gelaran ini dan jika mengharapkan mendapat U41, kita harus mengambil Ijazah Farmasi yang mana kita tahu amat sukar memperolehinya.
Itulah sebabnya saya menyatakan kita harus ada 'approach' baru dalam perjuangan.
Kita tidak boleh lagi menentang arus. Perkara paling penting jika ingin mengembangkan profesion ini ialah kita harus melakukan sesuatu supaya diterima oleh Pegawai dan Bahagian Perkhidmatan Farmasi secara amnya dengan ikhlas hati. Sekiranya ini berlaku, apa-apa tuntutan kita akan menjadi mudah untuk dipertimbangkan.
Kita tidak harus sesekali melakukan sesuatu yang bersifat menentang atau memberi kesan negatif kepada profesion mereka. Kita seharusnya berada dalam satu keluarga yang mesra, baik, bekerjasama dan bersama-sama memperutuhkan perkhidmatan Farmasi yang berkualiti secara total. Inilah yang harus menjadi pegangan dan matlamat.
Oleh yang demikian saya berpendapat satu usaha baru harus dimulakan yang memfokuskan kepada hubungan baik antara Pegawai Farmasi dan Pen.Pegawai Farmasi dengan dimulakan oleh Kesatuan dan Bhg Perkhidmatan Farmasi.
Saya juga ingin menyentuh penubuhan Majlis Perundingan PPF.
Cadangan mengadakan Majlis tidak seharusnya dipandang negatif oleh Kesatuan mahupun Persatuan. Perjumpaan diantara semua organisasi yang ada hubungkait dengan profesion kita sangatlah penting dan menjadi media untuk berkomunikasi serta membantu menyelesaikan banyak masalah atau mempercepatkan sebarang cadangan pembangunan tanpa mengganggu perjalanan Pertubuhan itu sendiri.
Kesatuan dan Persatuan tidak seharusnya melihat penubuhan majlis PPF sebagai satu ancaman atau sindiran kepada tujuan penubuhan mereka. Seharusnya kita berbangga adanya Majlis ini dimana dapat kita bersemuka dengan semua PPF dan bekas PPF yang telah menjadi pengajar dan P.S.U di bahagian latihan.
Setiap perbincangan akan diatur dengan teliti supaya tidak menyentuh perjuangan pertubuhan itu masing-masing. Perlantikan wakil dari BPF juga tidak seharusnya dipandang negatif. Kedudukan beliau sangat penting dalam Majlis ini dimana banyak perkara boleh kita bincangkan dan perolehi maklumat. Beliau juga telah bersetuju memberi kerjasama baik dalam majlis ini. Sebagai pengerusi bukan bererti beliau akan mengawal semua ahli-ahli atau menyoal, tetapi lebih kepada perbincangan demi pembangunan profesion. Seharusnya dipandang dari sudut positif dan bukan melemparkan berbagai tuduhan negatif kepada beliau.
Saya sangat berharap semua PPF membuka minda dan berfikir secara positif masa hadapan kita dalam pengembangan profesion terutama dalam aspek pendidikan, karier, latihan dan kebajikan. Sama-samalah kita bersatu hati demi pembangunan profesion tanpa mengambil kira rasa ego dan pandangan negatif.
SAYA TETAP AKAN BERJUANG UNTUK SEMUA PPF TIDAK KIRA APA HALANGAN YANG DITEMPUHI SEHINGGA BERJAYA!
Salam mesra.
Saturday, September 22, 2018
SKIM BERSEPADU PENOLONG PEGAWAI FARMASI
Salam sejahtera semua Penolong Pegawai Farmasi Malaysia
Kita amat bersyukur kerana semua usaha kita untuk dinaikkan ke Skim Bersepadu sejak 2016 hampir mencapai kejayaan.
Bermula dari Usaha Task Force PPF diketuai En.Laurunce Vun pada 2016, mantan Ketua Profesion Tn.Hj.Abu Bakar dan pengganti beliau Pn.Faridah Saidi serta PPF di BPF KKM Hj.Kamal, En.Indra Shahril dll, Exco Kesatuan dikemudi oleh Presiden Hj.Razali Dollah, Hj.Rozali Jaafar, SU Hj.Rahim dan semua Exco2 bertungkus lumus bersama-sama berusaha memastikan Kertas Kerja Skim Bersepadu cukup mantap dan diterima oleh Pengarah Kanan Bhg Perkhidmatan Farmasi dan seterusnya diangkat kepada Bhg Sumber Manusia KKM.
Baru-baru ini klita telah berjaya menjalankan Pemurnian Kertas Kerja Sik Bersepadu kali ke 3 di Maktab Penjara Kajang selama dua hari.
Kita harapkan Kertas Kerja ini juga akan diterima oleh JPA dan diluluskan Skim baru ini dalam masa terdekat. Sama-sama kita berdoa untuk berita baik yang dinanti-nantikan sekian lama. Buat mnasa ini kita telah mempunyai lebih dari 100 PPF yang mempunyai Ijazah dan Master.
ALL THE BEST TO OUR PROFESION.
Kita amat bersyukur kerana semua usaha kita untuk dinaikkan ke Skim Bersepadu sejak 2016 hampir mencapai kejayaan.
Bermula dari Usaha Task Force PPF diketuai En.Laurunce Vun pada 2016, mantan Ketua Profesion Tn.Hj.Abu Bakar dan pengganti beliau Pn.Faridah Saidi serta PPF di BPF KKM Hj.Kamal, En.Indra Shahril dll, Exco Kesatuan dikemudi oleh Presiden Hj.Razali Dollah, Hj.Rozali Jaafar, SU Hj.Rahim dan semua Exco2 bertungkus lumus bersama-sama berusaha memastikan Kertas Kerja Skim Bersepadu cukup mantap dan diterima oleh Pengarah Kanan Bhg Perkhidmatan Farmasi dan seterusnya diangkat kepada Bhg Sumber Manusia KKM.
Baru-baru ini klita telah berjaya menjalankan Pemurnian Kertas Kerja Sik Bersepadu kali ke 3 di Maktab Penjara Kajang selama dua hari.
Kita harapkan Kertas Kerja ini juga akan diterima oleh JPA dan diluluskan Skim baru ini dalam masa terdekat. Sama-sama kita berdoa untuk berita baik yang dinanti-nantikan sekian lama. Buat mnasa ini kita telah mempunyai lebih dari 100 PPF yang mempunyai Ijazah dan Master.
ALL THE BEST TO OUR PROFESION.
Friday, March 10, 2017
Top 15 Anti-Inflammatory Foods
https://draxe.com/anti-inflammatory-foods/
By Dr.Josh Axe


By Dr.Josh Axe

When we look at the diseases that plague our society — arthritis, heart disease, diabetes, high blood pressure, asthma, inflammatory bowel disease (IBD) — we see that long-term lifestyle changes are needed. What might not be as obvious is the common denominator tied to all of them and more: inflammation is at the root of most diseases.
By addressing the inflammation with anti-inflammatory foods, not only can the symptoms of these diseases be alleviated, but we could even see them cured.
Anti-Inflammatory Foods Can Transform Your Health
Inflammation as a bodily function is not necessarily a bad thing. When the body is injured or ill, the lymphatic (immune) system springs into action, bringing the immune system’s army of white blood cells to the area of concern via increased blood flow.
With the increased attention to the area, there might also be swelling, redness, heat, and pain or discomfort. You’ve probably seen this immune response in action, as a cut or scrape becomes hot and puffy around the wound while the extra blood runs. Inflammation, in a healthy body, is the normal and effective response that facilitates healing.
Sadly, we know this isn’t the whole story.
When the immune system overreaches and begins attacking healthy body tissues, we’re met with an autoimmune disorder like leaky gut and inflammation in otherwise healthy areas of the body. This is also the case for arthritis and fibromyalgia symptoms, as well as celiac and irritable bowel disease (IBD). For diseases that aren’t autoimmune, inflammation can still play a part as the body continuously tries to heal the tissues in a given area. Asthma creates inflamed airways; inflammation related to diabetes affects insulin resistance; and so on.
Despite the connection between inflammation and prevalent diseases, as well as the connection between diet and inflammation that we’ll explore, diet isn’t always analyzed in response to inflammation. In a 2014 study on diet and IBD, 33 percent of the patients in the study opted against the proposed anti-inflammatory diet. All of the patients who participated and consumed anti-inflammatory foods found enough relief that they were able to discontinue at least one of their medications. Still, the study notes that physicians typically offer “if it hurts, don’t do it” advice instead of clear dietary guidelines. (1)
Certainly, there is more we can do to promote anti-inflammatory lifestyle changes.
The Anti-Inflammatory Diet
Standard American diets (appropriately called SAD) are never touted as exemplary, but when talking about inflammation, it becomes vitally important to rethink our typical diets. As a report from the National Institute of Allergies and Infectious Diseases reported:
While today’s modern diet may provide beneficial protection from micro- and macronutrient deficiencies, our over abundance of calories and the macronutrients that compose our diet may all lead to increased inflammation, reduced control of infection, increased rates of cancer, and increased risk for allergic and auto-inflammatory disease. (2)
To move toward an anti-inflammatory diet and anti-inflammatory foods, we primarily move away from the abundance of overly processed, unbalanced diets of the West and toward the ancient eating patterns of the Mediterranean. (3) A Mediterranean diet comprises plenty of fresh fruits and vegetables, little to no red meat, certainly no chemicals or meat additives, and an abundance of omega-3 foods.
As we look into the anti-inflammatory components of certain foods and herbs, we can see how this kind of diet is linked with lowered inflammation. Among the many compounds found in fresh produce, a few general categories stand out as beneficial when attacking inflammation and inflammatory diseases at their source.
- Antioxidant foods
- Minerals
- Essential fatty acids
There’s little doubt that the pursuit of a healing diet begins with a menu high in vegetables, fruits, wild meats and sprouted seeds rich with omega-3 benefits. The evidence is clear that such anti-inflammatory foods can regulate the immune system and impact the way inflammation affects our bodies and our lives. (4)
Top 15 Anti-Inflammatory Foods
Small, gradual changes are typically more sustainable, easier for the body to adapt to and can make you less likely to go back to your old ways. So rather than emptying your pantry and sailing off to the Mediterranean, you can pursue an anti-inflammatory diet one step at a time.
By adding in the anti-inflammatory foods that fight inflammation and restore health at a cellular level, you can begin to repair the body without any drastic changes. Once you find foods that heal your body and satisfy your palate, you can remove the inflammation-causing offenders without feeling deprived. Let’s take a look at 15 of the best anti-inflammatory foods you can add to your diet.
1. Green Leafy Vegetables
The produce drawer is the first spot in your refrigerator or pantry to fill when fighting inflammation. Fruits and vegetables are rich in antioxidants that restore cellular health, as well as anti-inflammatory flavonoids. If you struggle to consume added portions of green leafy vegetables, try this delicious anti-inflammatory juice that incorporates greens alongside some of the strongest anti-inflammatory foods in the list.
Swiss chard nutrition, for example, is extremely high in the antioxidants vitamin A and C, as well as vitamin K, which can protect your brain against oxidative stress caused by free radical damage. Eating chard can also protect you against the common vitamin K deficiency.
2. Bok Choy
Also known as Chinese cabbage, bok choy is an excellent source of antioxidant vitamins and minerals. In fact, recent studies show that there are over 70 antioxidant phenolic substances in bok choy. These include something called hydroxycinnamic acids, which are robust antioxidants that scavenge free radicals. (5) A versatile vegetable, bok choy can be made in many dishes outside of Chinese cuisine, so make it one of your go-to anti-inflammatory foods.
3. Celery
In recent pharmacological studies, benefits of celery include both antioxidant and anti-inflammatory abilities that help improve blood pressure and cholesterol levels, as well as prevent heart disease. Celery seeds — which can be found either in whole seed form, extract form or ground-up — have impressive health benefits on their own, as they help to lower inflammation and to fight bacterial infections. It’s an excellent source of potassium, as well as antioxidants and vitamins.
Also, balance is the key to a healthy body free of inflammation. A good example of mineral balance tied to inflammation is the proper mix of sodium foods and potassium-rich foods. Sodium brings in fluid and nutrients, while potassium flushes toxins. We know that processed foods are high in sodium, but our SAD diets aren’t as rich in potassium. Without this pairing, toxins can build up in the body, once again inviting inflammation. One of the benefits of celery is that it’s an excellent source of potassium, as well as antioxidants and vitamins.
4. Beets
A marker of a food chock-full of antioxidants is its deep color, and beets are a prime example! The umbrella category of antioxidants includes a great deal of substances. In general, they fight to repair the cell damage caused by inflammation. In the case of beets, the antioxidant betalain gives them their signature color and is an excellent anti-inflammatory. (6) When added to the diet, beet benefits include repairing cells and adding high levels of inflammation-fighting potassium and magnesium.
Beets also contain quite a bit of magnesium, and a magnesium deficiency is strongly linked with inflammatory conditions. (7) Calcium, while a vital nutrient, is not processed well within the body without magnesium. When calcium builds up in the body, it becomes unwanted — this unpleasant buildup, such as calcified kidney stones, then invites inflammation. But when a balanced diet is consumed, with anti-inflammatory foods rich in calcium as well as magnesium, the body better processes what’s consumed.
5. Broccoli
The poster vegetable for healthy eating, it’s no secret that broccoli is a valuable addition to any diet. For an anti-inflammatory diet, it’s invaluable. Broccoli is high in both potassium and magnesium, and its antioxidants are particularly potent anti-inflammatory substances in their own right. (8)
Broccoli is an antioxidant powerhouse, with key vitamins, flavonoids and carotenoids. These work together to lower oxidative stress in the body and help battle both chronic inflammation and the risk of developing cancer. (9)
6. Blueberries
One antioxidant in particular stands out as an especially strong anti-inflammatory, and that’s quercetin. Found in citrus, olive oil and dark-colored berries, quercetin is a flavonoid (a beneficial substance or phytonutrient that’s prevalent in fresh foods) that fights inflammation and even cancer. (10) The presence of quercetin is one of the health benefits of blueberries.
In a study seeking treatment for IBD, an extract from the noni fruit was used to affect the gut flora and colon damage done by inflammatory diseases. Of the effects the extract had, quercetin created the prominent anti-inflammatory actions.
Another study found that consuming more blueberries slowed cognitive decline and improved memory and motor function. The scientists in this study believed these results were due to the antioxidants in blueberries protective the body from oxidative stress and reducing inflammation.
7. Pineapple
Usually, when it’s packaged in supplement form, quercetin is often paired with bromelain, a digestive enzyme that’s one of the benefits of pineapple. After being used for years as part of an anti-inflammatory foods protocol, bromelain is observed to have immune-modulating abilities — that is, it helps regulate the immune response that so often creates unwanted and unnecessary inflammation. (11)
Pineapple also helps improve heart health because of the effects of powerful bromelain. which can fight blood clotting and is nature’s answer to those taking an aspirin a day to lower the risk of heart attack. Bromelain has been shown to stop blood platelets from sticking together or building up along the walls of blood vessels – both known causes of heart attacks or strokes.
The benefits of pineapple are due to its high supply of vitamin C, vitamin B1, potassium and manganese, in addition to other special antioxidants that help prevent disease formation. Pineapple is filled with phytonutrients that work as well as many medicines do to reduce symptoms of some of the most common illnesses and conditions we see today.
8. Salmon
Salmon is an excellent source of essential fatty acids, and considered one of the best omega-3 foods. Omega-3s are some of the most potent anti-inflammatory substances, showing consistent relief of inflammation and reduction of the need for anti-inflammatory medications. (12)
Research shows that omega-3 fatty acids reduce inflammation and may help lower risk of chronic diseases, such as heart disease, cancer and arthritis. Omega-3 fatty acids are highly concentrated in the brain and appear to be important for cognitive (brain memory and performance) and behavioral function. (13)
The source of fish and meat among anti-inflammatory foods is a vital component. One of the dangers of farmed fish is it doesn’t have the same nutrients as wild-caught salmon.
9. Bone broth
Bone broths contain minerals in forms that your body can easily absorb: calcium, magnesium, phosphorus, silicon, sulphur and others. They contain chondroitin sulphates and glucosamine, the compounds sold as pricey supplements to reduce inflammation, arthritis and joint pain. (14)
When my patients suffer from leaky gut syndrome, I ask them to consume a lot of bone broth it contains collagen and the amino acids proline and glycine that can help heal leaky gut and the damaged cell walls of the inflamed gut.
10. Walnuts
When following a diet without a lot of meats, nuts and seeds can make up the difference for protein and omega-3s. Add omega-3-rich walnuts to green leafy salads drizzled with olive oil for a satisfying anti-inflammatory meal, or grab a handful for an on-the-go snack.
Phytonutrients can help protect against metabolic syndrome, cardiovascular problems and type 2 diabetes. And some phytonutrients in walnuts are hard to find in any other foods. (15)
11. Coconut oil
So much can be written about the way herbs and oils work together to form anti-inflammatory partnerships. Lipids (fats) and spices create strong anti-inflammatory compounds, especially coconut oil and the components of turmeric (see #15). (16) In a study in India, the high levels of antioxidants present in virgin coconut oil reduced inflammation and healed arthritis more effectively than leading medications. (17)
Also, oxidative stress and free radicals are the two biggest culprits of osteoporosis. Since coconut oil benefits include fighting such free radicals with its high levels of antioxidants, it’s a leading natural treatment for osteoporosis.
Coconut oil uses include topical preparations as well as culinary — and as a heat-stable oil, it’s excellent for sautéing anti-inflammatory vegetables.
12. Chia seeds
Fatty acids found in nature are more balanced than the fats we typically consume in our typical diets. Chia seeds benefits, for example, offer both omega-3 and omega-6, which should be consumed in balance with one another. (18)
Chia are an antioxidant, anti-inflammatory powerhouse, containing essential fatty acids alpha-linolenic and linoleic acid, mucin, strontium, vitamins A, B, E, and D, and minerals including sulphur, iron, iodine, magnesium, manganese, niacin, thiamine.
Chia seeds’ ability to reverse inflammation, regulate cholesterol and lower blood pressure make it extremely beneficial to consume for heart health. (19) Also, by reversing oxidative stress, someone is less likely to develop atherosclerosis when they’re regularly consuming chia seeds.
13. Flaxseeds
An excellent source of omega-3s and phytonutrients, flaxseeds benefits include being packed with antioxidants. Lignans are unique fiber-related polyphenols that provide us with antioxidant benefits for anti-aging, hormone balance and cellular health. Polyphenols support the growth of probiotics in the gut and may also help eliminate yeast and candida in the body.
Before you use them alongside your other new anti-inflammatory foods, consider grinding them in a coffee grinder to ensure the digestive tract has easy access to their many benefits. (20)
14. Turmeric
Turmeric’s primary compound, curcumin, is its active anti-inflammatory component. Documented for its affects against inflammation in numerous circumstances, turmeric health benefits prove invaluable in an anti-inflammatory diet. (21)
The journal Oncogene published the results of a study that evaluated several anti-inflammatory compounds. It found that aspirin (Bayer, etc.) and ibuprofen (Advil, Motrin, etc.) are least potent, while curcumin is among the most potent anti-inflammatory and anti-proliferative agents in the world. (22)
Due to its high anti-inflammatory properties, turmeric is highly effective at helping people manage rheumatoid arthritis (RA). A recent study out of Japan evaluated its relationship with interleukin (IL)-6, the inflammatory cytokine known to be involved in the RA process, and discovered that curcumin “significantly reduced” these inflammatory markers. (23)
15. Ginger
Used fresh, dried, or in supplement form and extracts, ginger is another immune modulator that helps reduce inflammation caused by overactive immune responses.
Ayurvedic medicine has praised ginger’s ability to boost the immune system before recorded history. It believes that because ginger is so effective at warming the body, it can help break down the accumulation of toxins in your organs. It’s also known to cleanse the lymphatic system, our body’s sewage system.
In fact, ginger health benefits may even include treating inflammation in allergic and asthmatic disorders. (24)
Inflammatory Foods to Avoid
With anti-inflammatory foods filling the diet, you naturally begin to eliminate pro-inflammatory foods and substances — they’re not as satisfying as a diet rich in whole foods.
A prime suspect is the duo of saturated and trans fatty acids. Found in processed foods, these fats cause inflammation and increase risk factors for obesity, diabetes and heart conditions. (25) The same foods are also likely to be higher in omega-6 fatty acids, which are necessary but only to an extent.
In excess and without the balance of omega-3s, omega-6 fats actually create inflammation in the body. Sadly, the University of Maryland Medical Center reports, “The typical American diet tends to contain 14–25 times more omega-6 fatty acids than omega-3 fatty acids.” (26)
Simple, refined sugars and carbohydrates are more inflammation-causing culprits. Limiting refined grains is an important factor in an anti-inflammatory diet. (27) Whole grains should replace the refined carbohydrates, as truly whole grains are important sources of nutrition. (28) Sourcing these grains as fermented sourdough allows the nutrients to be broken down and better available to the body. (29)
Finally, establishing a regular routine of physical activity can help prevent systemic inflammation from building up or returning. (30) An active life fueled by fresh, whole anti-inflammatory foods and unrestricted by processed, toxic compounds can set you on the path toward freedom from inflammation.
How to Reverse Cavities Naturally & Heal Tooth Decay
https://draxe.com/naturally-reverse-cavities-heal-tooth-decay/
by Dr.Josh Axe





by Dr.Josh Axe

There is a common belief today about cavities that once you have tooth decay, that cavity can NOT be reversed. Then the only solution to oral wellness is to have part of your tooth drilled out and filled with a synthetic material. However, it’s been proven that there are ways to reverse cavities naturally.
In fact, according to a study published in the British Medical Journal, cavities and tooth decay could potentially be reversed with diet. (1)
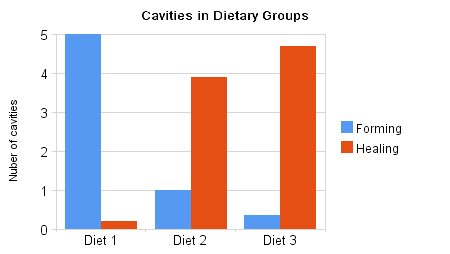
A study was performed on 62 children with cavities, and they were divided into three different diet groups. Group 1 ate a standard diet plus oatmeal (rich in phytic acid). Group 2 consumed a normal diet and supplemented with vitamin D. Group 3 ate a grain-free diet and took vitamin D.
The results found that Group 1 who had a diet high in grains and phytic acid had an increase in cavities. Group 2 had improvements in cavities and less form. Group 3, who followed a grain-free diet with nutrient-rich foods like vegetables, fruits, meat, milk and took vitamin D, saw the greatest improvements — nearly all cavities were healed. (2)
This study, along with the backing of many doctors and dentists, proves we have been misinformed about what causes cavities and how to reverse cavities naturally.
Dentist Ramiel Nagel, who authored the book “Cure Tooth Decay,” has helped many of his patients “reverse” their tooth decay and would rather not put in dangerous amalgam fillings. He believes that you can prevent cavities with nutrient-rich foods.
In this article, I am going to go over the causes of tooth decay and how it may be prevented and in many cases even reversed.
The Cause of Tooth Decay
To understand the link between diet and oral wellness, we must start with one of the most well-respected dentists who ever lived, Weston A. Price.
West A. Price lived in the early 1900s and was the chairman of the National Dental Association (1914–1923) and a pioneer for the American Dental Association (ADA).
Weston Price traveled the world searching to discover what causes tooth decay. Dr. Price found a common link between eating modern foods and cavities. He witnessed that many indigenous isolated tribes had perfect teeth and little tooth decay. But once they were exposed to a Western diet, they experienced tooth decay, bone loss and chronic illness.
According to the ADA, this is the cause of tooth decay:
“[Tooth decay] occurs when foods containing carbohydrates (sugars and starches) such as milk, pop, raisins, cakes or candy are frequently left on the teeth. Bacteria that live in the mouth thrive on these foods, producing acids as a result. Over a period of time, these acids destroy tooth enamel, resulting in tooth decay.”
But the truth is the ADA is only hitting on one of the four things that can contribute to tooth decay.
According to the insights of Dr. Edward Mellanby, Dr. Weston Price and Ramiel Nagel, there are four main things that contribute to tooth decay: (3)
- Lack of minerals in the diet (calcium deficiency, magnesium deficiency and phosphorus deficiency)
- Lack of fat soluble vitamins (A, D, E and K, especially vitamin D deficiency)
- Too much consumption of phytic acid-rich foods
- Too much consumption of processed sugar
Let’s discuss the four aspects that cause tooth decay and how they can be addressed with diet, along with ways to reverse cavities naturally.
How to Reverse Cavities Naturally
Don’t be fooled, in addition to brushing and flossing daily, there are several ways you can reverse cavities naturally and maximize your oral health without resorting to taking in fluoride. Here are just a few ways to reverse cavities naturally for you to consider, while also avoiding fluoride:
1. Remove Sugar
Probably the worst culprit of them all for anyone who desires healthy, cavity-free teeth, sugar should be avoided like the plague. So kick that sugar addiction stat. Not only does sugar feed oral bacteria that prevents a healthy flow of dental fluids, but it’s highly acidic and can literally decalcify or demineralize the structural content of teeth that create dental decay. (4)
This means staying away from soda, candy and baked goods with sugar. Additionally, use raw honey and maple syrup, and drink juices sparingly, as too much sugar can contribute to cavity formation. Be careful of artificial sweeteners because of their health risks as well. Bottom line: Make stevia your new best friend along with raw honey in moderation!
2. Eliminate Phytic Acid
Phytic acid (phytate) is a mineral blocker and enzyme inhibitor found in grains, nuts, seeds and beans that can cause serious health problems in our diets. The main reason phytic acid has become an issue today is because we have stopped ancient food preparation techniques, such as sprouting or sourdough fermentation, which kills off the phytic acid.
According to research published in the The Lancet, a diet high in phytic acid creates mineral deficiencies and causes osteoporosis. About 80 percent of phosphorus in grains and beans is bound to phytic acid so it’s completely unabsorbable. In addition to blocking phosphorus availability in humans, these molecules bind minerals necessary for oral health, such as calcium, magnesium, iron and zinc — thus causing them to be unavailable for proper utilization. Consuming foods high in phytic acid decreases magnesium absorption by 60 percent and zinc by 20 percent. (5)
Phytic acid not only prevents you from absorbing minerals in your food, but it also leaches minerals out of your body, bones and teeth! (6)
Subsequently, the powerful anti-nutritional effects of phytic acid have been known to cause digestive disorders, lack of appetite, nutrient deficiencies and tooth decay. A good rule of thumb is to limit your grain consumption and stay completely clear from unfermented soy products. (7)
Because phytic acid is much higher in foods grown using modern high-phosphate fertilizers than those grown in natural compost, try to only eat foods that are organic and GMO-free.
If you’re aiming to improve your health and reverse cavities naturally, foods high in phytic acid like grains, beans, nuts and soy should be avoided. However, if you soak grains or nuts and then sprout them or do sourdough fermentation, you can reduce phytic acid by around 50 percent to 100 percent. (8)
3. Consume Raw Dairy and Nutrient-Rich Foods
Raw dairy is filled with the vitamins and minerals that contribute to a healthy dental fluid flow and help maintain strong teeth and promote oral wellness. Thus, it’s a great way to get cavity-free teeth. Loaded with calcium, vitamin K2, vitamin D3, magnesium, phosphorus and fat-soluble vitamins, it’s a good idea to consume raw dairy products at least weekly. I recommend goat milk kefir, raw cheeses and organic grass-fed butter as great options.
Remember, if you’re going to beat tooth decay, you need to increase your fat-soluble vitamin intake and mineral intake. If I were creating an ideal diet to follow, it would look like this:
- Rich in animal foods like bone broth, meat, fish and eggs.
- Raw and cooked vegetables, especially green leafy vegetables.
- Raw dairy like kefir, cheese and grass-fed butter.
- Fruit, one piece daily early in day.
- Vitamin D — get plenty of sunshine, and days not in sun supplement with 5,000IU daily of D3.
- Foods high in healthy fats like coconut oil, avocado, olives, and fish or fermented cod liver oil.
- Fermented grains only and in moderation, such as true sourdough bread (or even better no grains at all). You can buy raw flours and breads.
- Nuts, seeds and beans only that have been sprouted.
- Finally, NO processed foods, packaged foods or fast food.
4. Use Mineralizing Toothpaste
First of all, I know it can get expensive, but there are several brands of fluoride-free toothpaste that you won’t have to pay a small fortune to get your hands on. Second, if you’re looking to save a buck or two and also want to remineralize your teeth in a particularly powerful way, try making your own Homemade Remineralizing Toothpaste:
- 4 tablespoons coconut oil
- 2 tablespoons baking soda (aluminum-free)
- 1 tablespoon xylitol or 1/8 teaspoon stevia
- 20 drops peppermint or clove essential oil
- 20 drops trace minerals or (calcium/magnesium powder)
5. Try Oil Pulling
Used for centuries by Ayurvedic medicine, oil pulling is a fantastic oral detoxification procedure that has gained some popularity in the U.S. the last several years. Simply done by swishing a tablespoon of oil in your mouth for 20 minutes, this simple oral detoxification procedure has been praised to cure everything from gingivitis to headaches to systemic diseases like diabetes.
If you can’t do 20 minutes, three to five minutes is still good. I recommend using coconut oil or MCT oil and a drop or two of clove and/or tea tree essential oils for maximal antiseptic and antifungal power. Here are some tips:
- The best time to oil pull (like most other detoxification procedures) is first thing in the morning right after you get out of bed.
- Don’t let the 20-minute time frame deter you. You won’t even notice 20 minutes have gone by if you do this during your normal morning routine (i.e., while you shower, put your clothes on and prep for the day).
- I then recommend that you spit the spent oil in the trash rather than into the sink, as an accumulation of oil could pose problems for household plumbing down the road.
- Immediately afterward, rinse your mouth out with warm water. Use salt water for added antimicrobial properties.
- Don’t be shocked if the oil/saliva mixture you spit out is milky white or yellow.
- Finally, brush your teeth as normal.
Note: This should be a relatively relaxing process, so don’t feel compelled to vigorously swish your mouth with oil for the entire time or else you’re bound to get sore jaw muscles. Simply and gently move the oil in your mouth and through your teeth without swallowing any of it.
Takeaways on How to Reverse Cavities Naturally
- According to the insights of Dr. Edward Mellanby, Dr. Weston Price and Ramiel Nagel, there are four main things that contribute to tooth decay: lack of minerals in the diet (calcium deficiency, magnesium deficiency and phosphorus deficiency); lack of fat soluble vitamins (A, D, E and K, especially vitamin D deficiency); too much consumption of phytic acid-rich foods; and too much consumption of processed sugar.
- You can reverse cavities naturally by removing sugar, eliminating phytic acid, consuming raw dairy and nutrient-rich foods, using mineralizing toothpaste, and try oil pulling.
In a nutshell, these are the best ways to naturally reverse cavities. Take charge of your oral wellness today, and show off your new, healthy smile with pride!
Subscribe to:
Posts (Atom)